Dr Ron Whelan top take-aways on SA's vaccine rollout, new COVID-19 variants and staying safe in

We've all heard people refer to the time periods relating to isolation for those who contract COVID 19, or quarantine for those are exposed to the disease. But how well do we understand how long it might take to recover from COVID 19 - and how period differs between individuals?
Discovery is currently at the centre of helping South Africa to accelerate vaccine procurement:
- Discovery Group CEO, Adrian Gore, is leading the National Vaccines Acquisition Task Team, reporting directly to the Minister of Health and supporting the coordination of financing and procurement of vaccines for South Africa.
- O READ MORE: ADRIAN GORE, DISCOVERY CHIEF EXECUTIVE, SHARES DISCOVERY'S POSITION ON SOUTH AFRICA'S COVID-19 VACCINATION PROGRAMME (PUBLISHED 15 FEBRUARY)
- Various Discovery senior executives are also working alongside government and private sector colleagues to get COVID-19 vaccines into the country as quickly as possible and to help ensure that South Africa is ready to implement a highly effective vaccine rollout process.
"At Discovery, we have had three priorities throughout the COVID-19 pandemic: protect our people, protect our clients and support South Africa," says Dr Ron Whelan, Discovery Health's chief commercial officer and head of the company's COVID-19 Task Team.
"Discovery has provided pro bono support to the National Department of Health in the development of the country's Bluetooth contact tracing app, COVID Alert SA. This initiative, together with our current involvement in the country's vaccine programme, speaks to the heart of our core purpose - making people healthier and enhancing and protecting their lives."
Staying safe in 2021? Think of the COVID-19 virus on the tip of a sewing needle
"We can use a simple analogy to demonstrate the need to adhere to preventive measures for the foreseeable future. The tip of a sewing needle may seem miniscule, yet it could accommodate 10 000 COVID-19 virus particles on its 1 mm surface. If you were then to blow onto the tip of the needle, you could imagine those microscopic viruses would be dispersed into the air to later drop onto the ground or a surface or be inhaled," explains Ron.
"This is like blowing onto a dandelion parachute and causing the filaments to be propelled into the air. And, this is what happens when we are infected with COVID-19 and speak, cough, sneeze or exhale without taking precautions to prevent the spread of the exhaled droplets. Mask-wearing, handwashing and social distancing work to limit our exposure to these tiny viral particles in the air or on surfaces around us."
"We all have an obligation to our family, friends, colleagues and communities to continue adhering to preventive measures while we wait for our vaccine programme to ramp up to the point at which we hope to achieve population immunity," says Ron.
- Keep reading for details on South Africa's vaccine rollout programme and achieving population immunity.
Staying safe in 2021? Imagine layers of Swiss cheese!
"Another powerful way to understand the power of COVID-19 preventive measures is through Australian virologist Professor Ian Mackay's 'Swiss cheese model'," adds Ron. "He suggests that each preventive measure may be imperfect on its own - porous so to speak, like Swiss cheese - so the virus may get past a mask that we might touch with dirty hands. However, stacking preventive measures one after the next causes a powerful, exponential protective effect. Vaccination is the last layer of 'cheese' in this regard. Employers might consider helping their people to understand the importance of their behaviours through this model."
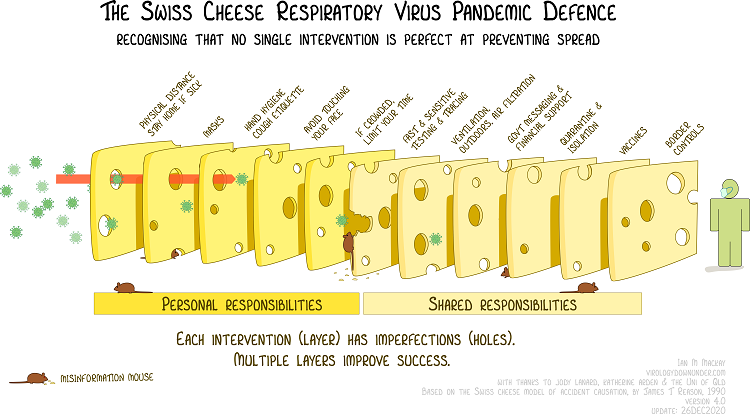
Source: Ian M. Mackay (virologydownunder.com) and James T Reason. Illustration: Rose Wong.
- Read our detailed article about the power of stacking preventive measures through the 'Swiss cheese model of Pandemic Defence'.
COVID Alert SA app has the power to prevent outbreaks and keep people safe
"Another powerful tool in our arsenal against COVID-19 is the choice to to download and use the COVID Alert SA app, and to encourage our loved ones to do the same," adds Ron. "This user-friendly app ensures absolute privacy while keeping every user notified (in as close to real time as possible) about their exposure to COVID-19. The app does not track location, and app users remain 100% anonymous at all times. This tool has the power to prevent outbreaks of COVID-19 and keep people safe, with protective consequences for society at large."
South Africa's second wave of COVID-19 infection
What does history teach us about second (and third) waves of infection?
The peak of South Africa's second wave of infection saw twice as many daily new infections as in our first wave. The second wave also had a much sharper peak - so cases escalated far faster than in the first wave.
- Later in this article we explain the increased "transmissibility" of South Africa's new COVID-19 variant.
Daily new infections are currently decreasing.
- Later in this article we explain the increased "transmissibility" of South Africa's new COVID-19 variant.
"It's funny how history repeats itself," says Ron. "The Spanish flu pandemic of 1918 and 1919 featured three waves of infection in the UK. Their first wave came in June and July 1919, then a second wave (significantly higher than the first) in Oct and Nov 1918, and a third in March 1919 (with cases higher than in the first wave but lower than the second wave). It's uncanny how the UK's recent experience of the COVID-19 pandemic has followed a very similar same pattern. While we hope to avert a third wave in South Africa and must do everything possible to prevent this, there is a very real risk of third wave. In both the UK and in Ireland, after cases of infection linked to the second wave had started decreasing, cases increased yet again, pushing these countries into their third waves of infection."
How much did hospital admissions of medical scheme members increase in the second wave?
Discovery Health's hospital admission data show that, in the first wave, new admissions to hospital peaked at 300 per day, compared to 520 per day in the second wave (up 70% on the first wave).
"At Discovery Health, we truly felt this massive increase in admissions - especially as infections rose in close succession over a matter of three to four weeks across the Eastern Cape, Garden Route, Cape Town, KwaZulu-Natal and Gauteng, in the last week of 2020 and first week of 2021. At this time, we were moving patients around the country to secure hospital and ICU beds and we were very concerned about the availability of ventilators and supplemental oxygen. This period pushed our healthcare system to the brink. The sheer scale of the second wave required a huge effort on our part, and on the part of partner hospital groups, to ensure that every medical scheme member who needed a hospital bed had access to one."
By the end of January, admissions decreased 23% from the peak of the second wave in December. And, as Ron adds, "We are tracking towards first-wave peak daily hospital admission levels. However, ICUs - and the health system more broadly - remain under tremendous pressure and we must continue vigilance."
Improved mortality rates: Benefit of our learning curve
"Any life lost is a tragedy. It is important to note, however, that among members of the 19 schemes administered by Discovery Health, we have managed to keep case fatality rates low through the pandemic. Member mortality rates have been around 1.9%, where the national average is at 2.7%. This is testimony to the exceptional work our physicians and healthcare workers have done during the pandemic."
It is interesting to look back at COVID-19 deaths in 2020 and to see that from May to June 2020 mortality rates dropped off significantly - by 25%. Ron attributes this to South Africa's early national lockdown, which allowed the healthcare system time to prepare, delayed the peak of the first wave of the pandemic by approximately 75 days, and allowed time for the science to emerge around how best to treat COVID-19. "We have since kept a steady case fatality rate," he adds.
Demystifying the COVID-19 variants that have recently emerged
Why was a COVID-19 viral variant detected in SA?
"South Africa has picked up a lot of press and attention linked to the announcement of the variant identified in our country," says Ron. "In fact, the reason it was detected is that South African scientists actively look for variants and do so on an ongoing basis. We do genomic sequencing on the virus and look for changes in its genetic code. We do this to stay ahead of the virus. So do the British and Brazilians. Other countries, such as the USA, do less of this work. This is why South Africa, the UK and Brazil are in the spotlight for variants having originated in these areas."
- Did you know that routine genomic surveillance of SARS-CoV-2 (the virus that causes COVID-19) is performed by a network of laboratories around the country? This Network for Genomic Surveillance South Africa, NGS-SA detected the new variant.
Three COVID-19 variants are currently dominant in the world:
- B.1.1.7 (UK variant) with 23 mutations, currently found in 62 countries
- 501Y.V2 (South African variant) with 21 mutations in 26 countries
- P.1 variant (Brazil) with 17 mutations in 7 countries
However, they all feature very similar mutations as they all have changes to the parts of the viral genetic material that tells the virus how to make the outer spike protein layer. This is explained below.
Why do variants originate?
Viral variants originate all the time, and are typical of pandemics. To understand this, we need to look at the structure of the COVID-19 virus (which is called SARS-CoV-2).
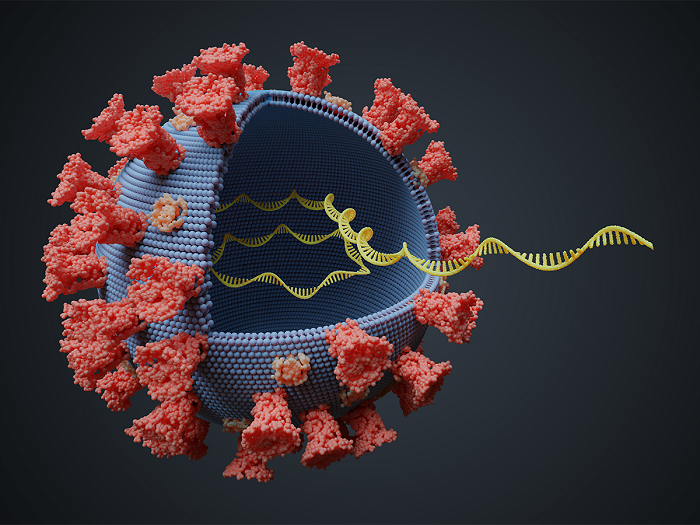
The COVID-19 virus is unique in that it has a protein and lipid shell (fatty layer that is dissolved with soap and water or alcohol), surrounded by spike proteins that are shown in red in the image above. These spikes land on and attach themselves to our cells when we are infected with COVID-19. Then the virus can inject its RNA into our cells, and this is how it reproduces itself and spreads.
The image above shows the virus and its RNA (ribonucleic acid, the virus's genetic material) in yellow in the middle. We can think of each RNA strand as a strand of information - like a strand of letters that make up certain words and together make up a sentence that carries an instruction. When the virus reproduces itself, it copies the code, or sentence, from the parent virus to the new one. But the virus lacks a 'spell check mechanism' and sometimes letters change - randomly - in the sentence when they are being 'rewritten' from one virus to the next. We call these subtle random changes mutations. They subtly change the way the virus works and can be positive or negative for the virus. The changes can be minor but still cause a significant change in the genetic code, which means a significant change to the physical features of the virus.
What do these mutations mean for the pandemic and for our second wave?
The new variants that have become dominant have caused mutations on the parts of the RNA that give instructions on how to make the spike protein. These changes have made these proteins more effective at attaching to our cells when we are infected.
"The virus has become, on average, 50% more transmissible. So, it spreads faster between people. This possibly accounts for the higher peak of infections experienced in our second wave," explains Ron. "The good news is that none of these variants seem to result in higher risk of death."
"However, as a very interesting analysis from the London School of Tropical Hygiene shows, the variant is more infectious, so it affects greater proportion of the population more quickly. This means that there is the potential for more people to be infected faster. The results in more deaths is due to the sheer increase in number of people contracting COVID-19 and not because the virus is more deadly. And, we have felt this in our second wave of infection "
"We are likely to see these variants spread to more countries over time. We are also likely to see more variants develop over time and our genomics researchers will stay on top of identifying them."
- New COVID-19 variant identified in South Africa: Here's what you need to know
How will South Africa's vaccine rollout programme rollout plan work?
Phase 1 will prioritise 1.2 million frontline healthcare workers for vaccination. Healthcare workers will be vaccinated primarily at district level (public and private hospitals). Additional community vaccination hubs will likely also be established to support the vaccination of GPs and healthcare workers who work outside of hospitals in the community.
Phase 1 will prioritise:
- 2 500 00 essential workers (teachers, police officers, miners, municipal workers and other frontline personnel, including people who work in security, retail food, banking and also home affairs, border control and port services)
- 1 100 000 people in institutions like care homes, old-age homes, shelters and prisons, and people who work in hospitality and tourism and at educational institutions.
- 5 000 000 people over 60 years of age
- 8 000 000 people over the age of 18 who have co-morbidities. This includes people who have either uncontrolled diabetes, chronic lung disease, poorly controlled cardiovascular disease, renal disease, HIV, tuberculosis (TB) and/or obesity.
Phase 3 will involve vaccinating the remaining adult population of approximately 22.5 million people.
"By the end of Phase 3, it is expected that 40 million South Africans (representing 67% of the population) will have had access to vaccination. At this level of vaccine coverage, we hope to achieve population immunity," says Ron.
"South Africa needs 56.5 million doses to vaccinate 40 million people. This number of doses accounts for that fact that our country has procured a mix of double-dose and single-dose (Johnson & Johnson) vaccines."
We are working hand in hand with colleagues across provincial and national Departments of Health to drive and ensure, first and foremost, equitable access to vaccines in our private and public healthcare systems."
- Note: None of the current COVID-19 vaccines have been tested on or are authorised for use on people under age 18 (for children). There are currently trials under way to extend vaccines to children aged 12 and above. And, for children under age 12, data on vaccine safety and efficacy will only emerge in 2020. All in all, we will not be immunising children at all in 2021 and review the situation thereafter.
- Read our full article on South Africa's vaccine rollout plan.
How will we fund South Africa's vaccine rollout programme?
Funding will come from government, possibly from medical schemes and business.
"We are working with the National Department of Health on stock allocation to public and private healthcare channels. Once the stock is in the private sector, it will go to private providers, mass vaccination sites, retail pharmacies, hospitals and more. Public providers will include state hospitals and clinics, and there is extensive work in the public sector on building out these platforms," says Ron.
"Leaders, managers and employees within businesses will be vaccinated according to the prioritisation outlined in the phases of the national rollout plan. Importantly, no one can be forced to be vaccinated. While it's highly recommended that everyone gets vaccinated, it's not compulsory," adds Ron.
A look at global vaccine rollout processes currently at play
The Moderna vaccine was the first vaccine to be granted approval globally. It is manufactured in the USA by a Boston-based company and comes in a little box containing 10 vials.
"The box is about the same size as a sleeve of three golf balls. Each of the vials in the box contains 10 vaccine doses. So the contents of each box are sufficient for 100 people to receive a single vaccine dose," says Ron. "To give you a sense of how expensive these vaccines are, this box will cost the equivalent of about $3 000, or R45 000 to R50 000. Fortunately, where the Moderna vaccine costs about $30 per dose, the Pfizer-BioNTech vaccine comes in at $10 to $15 or so per dose, and the AstraZeneca-Oxford vaccine costs $3 to $5 per dose."
"Regardless of the price of each vaccine, we need them. They therefore become affordable at any price point, given their effect on our people, society and economy."
Across the world, multiple countries are in the early stages of vaccine rollout, with the UK having converted cathedrals into mass vaccination sites. The USA has done the same at sports stadia and malls. "The USA is achieving close on 1 million vaccinations per day (5% of the population vaccinated by end of January 2021), but with their population of over 300 million people" adds Ron. "The UK has a faster rollout programme and is vaccinating approximately 400 000 people per day. By the end of January, they had vaccinated about 6% of the population."
"We are learning from the American and European experience and we will be able to drive an efficient programme on the back of these insights. In South Africa, we would like to get to 300 000 to 350 000 vaccinations per day. While it will take time to achieve these levels of daily vaccination, other countries have demonstrated that a fast ramp-up is achievable. For example, the UK and Israel ramped up to 400 000 and 165 000 vaccinations per day, respectively, in less than six weeks from the start of their programmes. As a result, Israel had vaccinated almost 60% of its 8 million-strong population by the first week in February."
How rapidly is global vaccine development progressing?
Globally, there are many potential vaccines in the pipeline:
- Over 154 vaccines in pre-clinical trial phase
- vaccines in phase 1 clinical trials
- vaccines in phase 2 clinical trials
- 22 vaccines in phase 3 trials (human trials with anywhere from 30 000 to 60 000 trial participants)
- 10 vaccines authorised and licensed for general use, with good production on these vaccines, which should allow us to vaccinate 1.5 billion people across the world (two doses each) in 2021
"Together, the main vaccine manufacturers aim to produce around 8 billion doses annually, providing access to vaccines for approximately 4 billion people globally. This gives us a sense of the scale of the programme and the speed at which things are moving," explains Ron.


All medical information found on this website including content, graphics and images, is for education and information objectives only. Discovery publishes content to help to promote a better understand of COVID-19 and COVID-19 vaccinations. The content covered is an overview of key concepts and is not exhaustive in nature. We encourage further reading from other credible sources where necessary.
South African organisations:
- National Department of Health's dedicated COVID-19 portal: https://sacoronavirus.co.za/
- National Institute for Communicable Diseases' (part of the National Health Laboratory Service) dedicated COVID-19 hub
- South African Health Products Regulatory Authority (SAPRHA - part of the National Department of Health).
- South African Medical Research Council (SAMRC)
- South African Medical Journal (SAMJ)
International Organisations:
- Johns Hopkins University
- Harvard Health, Harvard University COVID-19 resource center
- Mayo Clinic COVID-19 resource center
- New England Journal of Medicine (NEMJ)
- US Centers for Disease Control and Prevention (US CDC)
- US Food and Drug Administration (US FDA)
- World Health Organization (WHO)