Long COVID symptoms, impact on carrying out daily activities: Survey of just over 7,000 medical scheme members reveals key insights

An alarmingly high number of medical scheme members have protracted COVID-19 symptoms (long COVID), often with disruption to daily living. The risk of these events is higher in women, in those admitted to hospital or ICU for COVID-19, and those with high morbidity and pre-existing chronic illness. Being COVID-19 vaccinated and regular physical activity lower this risk.
Authors
Shirley Collie (Chief Healthcare Analytics Actuary, Discovery Health), Lizelle Steenkamp (Senior Healthcare Statistician, Discovery Health), Lebohang Radebe (Data Scientist, Discovery Health), Dr Smybinn Mathews (Clinician, Discovery Health) and Dr Dave Jacobs (Senior Clinician and Clinical Classification System Architect, Discovery Health)
"10%-20% of people experience a variety of mid- and long-term effects after they recover from their initial illness." What is post COVID-19 condition?
The World Health Organization (WHO) states that, "Most people who develop COVID-19 fully recover, but current evidence suggests approximately 10%-20% of people experience a variety of mid- and long-term effects after they recover from their initial illness. These mid- and long-term effects are collectively known as post COVID-19 condition or 'long COVID'."
The WHO goes into more detail in the following definition: "Post COVID-19 condition occurs in individuals with a history of probable or confirmed SARS CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms include fatigue, shortness of breath, cognitive dysfunction but also others, and generally have an impact on everyday functioning. Symptoms may be new onset following initial recovery from an acute COVID-19 episode or persist from the initial illness. Symptoms may also fluctuate or relapse over time."
Multiple medical institutions and scientific journals1,2,3,4 have reported that many recovered COVID-19 patients experience ongoing symptoms post the acute phase of their illness. Some patients report significant negative effects to their ability to perform day-to-day activities.
Research released on 27 May 2022 by the US Centers for Disease Control and Prevention (looking at a large cohort of US adults) estimated that up to 20% of people infected with COVID-19 are at risk of long COVID. More specifically they find that one in five COVID-19 survivors aged 18 to 64 and one in four survivors aged 65 years and over, experience at least one persistent symptom or health condition, four weeks after acute COVID-19, that is probably the result of having had COVID-19. These range from respiratory and musculoskeletal conditions (most common) to neurological conditions, kidney failure, cardiovascular conditions, blood clots and vascular issues.
As we go through waves of COVID-19 infection with highly transmissible COVID-19 variants, the number of people infected with SARS-CoV-2 increases, upping the numbers who could suffer post-COVID conditions.
Our aim - describe medical scheme member experience of long COVID, and look at what increases risk of this happening
Here we explain our approach to analysing Discovery Health Medical Scheme (DHMS) member-reported outcomes post a first documented COVID-19 infection.
We report back on:
- The most common reported post COVID-19 symptoms
- Reported changes in members' ability to undertake the normal activities of their daily lives
- A statistical modelling approach for identifying factors that lead to increased risk of either post COVID-19 symptoms or changes in activities of daily living.
Our approach - perception survey sent to scheme members
We emailed a 'COVID-19 symptom' digital survey to DHMS members who had recovered from documented, prior COVID-19 infection (confirmed by pathology PCR test results or through doctors' diagnosis, also based on doctor's access to patient PCR test results) between 1 March 2020 and 30 November 2021.
To create our COVID-19 symptom survey, we adapted and modified the National Institute for Communicable Diseases' (NICD) Long COVID-19 Survey7. We used this to capture member-reported symptoms post COVID-19 infection and to understand the challenges of daily living experienced post infection.
We obtained ethics approval for the survey from Human Research Ethics Committee at the University of the Witwatersrand.
Our COVID-19 symptom survey was emailed to DHMS medical scheme members who met the following criteria:
- Adult - over the age of 18
- A valid email address
- Laboratory- or clinician-confirmed COVID-19 infection between 1 March 2020 and 30 November 2021
- Recovered from COVID-19 infection
- No withdrawal from DHMS post infection
- No mortality post infection
We sent out the survey request via email in early December 2021, including a hyperlink to the survey itself.
Members were asked:
- About symptoms they experienced in the seven days prior to answering the survey questions.
Using their confirmed COVID-19 infection date, we calculated the time since recovery from COVID-19 for each participant. - To compare their ability to carry out activities of daily living before and after their COVID-19 infection.
It is important to note that any symptoms respondents experienced - not only those typical to post-COVID condition - were recorded.
Analysis of data from just over 7,000 respondents
We sent out 245,591 emails and received 9,403 responses (response rate of 3.8%).
We narrowed these down to 7,097 post COVID symptom responses, within which 5,537 responses also related to effects on ability to carry out daily activities.
We excluded:
- Members who'd had multiple documented COVID-19 infections as their experience was unique (and requires its own analysis as to the impact of repeat infection on long COVID)
- Incomplete survey responses were excluded
Most people in the post COVID symptom response group, 83% of the 7,097 respondents, had not been admitted to hospital for COVID-19 treatment.
The median follow-up time from recovery to survey completion date was 5.4 months.
This was the distribution of responses, in months since recovery:
- 1% of our members responded at two months post recovery
- 38% responded between three- and five-months post recovery, and
- 61% responded over six months post recovery
Our findings
1. The most common long COVID-19 symptoms experienced by medical scheme members
The most common symptoms reported in the 2 to 11 months since recovery from COVID-19 infection are shown in the graph below (Figure 1) and as follows:
- Headaches - 31% of respondents reported headaches. However, we excluded "headaches" from further analysis as headaches are commonly reported and likely to have been experienced prior to COVID-19 infection.
- Breathlessness (14%)
- Problems sleeping (14%)
- Dizziness (12%)
- A lack of concentration (11%)
- Muscle weakness (10%)
- Joint pain (9%)
Symptoms seem to be highest in two months post recovery. We see a decrease in symptoms from three months onward, but not all to pre-COVID levels where members were not experiencing the symptoms at all.
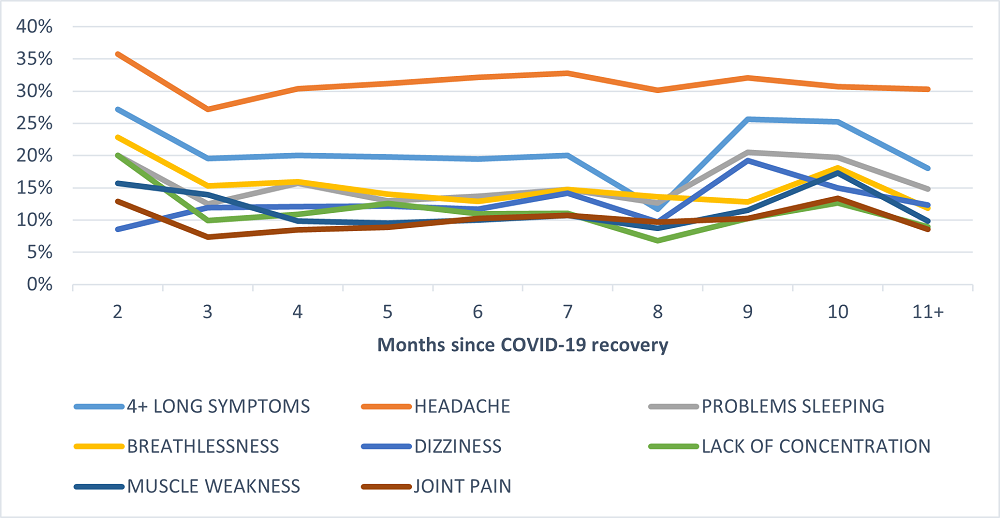
Figure 1: Most common symptoms post recovery from COVID-19 reported on by month since recovery
2. After acute COVID-19, effects on member ability to undertake day-to-day activities
We analysed members reporting on a deterioration in their ability to perform key daily living activities, where a member had no problems with the activity before COVID-19 infection and reported some or much difficulty in this area post COVID-19 infection.
Across all the categories members reported deterioration in ability with the highest changes seen in:
- Impact on one activity of daily living (ONE_ADL_CHANGE) 43%
- Concentration (30% of members reported a deterioration for this activity)
- Walking (20%)
- Seeing (16%)
- Communicating (7%)
- Hearing (5%)
- Self-care (3%).
These changes are also presented per month since recovery in the Figure 2, below:
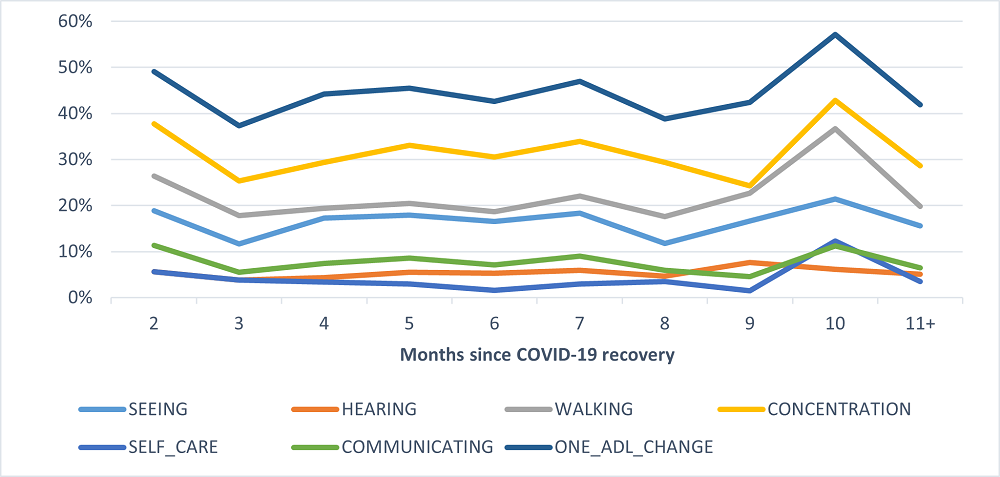
Figure 2: Deterioration reported in activities of daily living, by month, since recovery from COVID-19
3. Statistical modelling shows that being female, being admitted to ICU and having pre-existing chronic illness increases risk of long COVID.
Multivariate logistic regression analysis was performed to identify whether specific variables were associated with:
- Presence of long-COVID-19 symptoms
- Worsening in a person's ability to carry out the activities of daily living.
The risk factors considered in each of the models were:
- Age band (40, 40-64, 65+)
- Sex
- Chronic condition count (0, 1, 2, 3, 4+)
- COVID-19 vaccination status prior to infection (Fully vaccinated, partially vaccinated, unvaccinated)
- COVID-19 vaccination status post infection (None, 1 dose, 2 doses, 3 doses)
- Admitted or not admitted for acute COVID-19
- ICU stay during acute COVID-19 episode (yes/no?)
- Ventilation during acute COVID-19 episode (yes/no?)
- Number of symptoms reported during acute COVID-19 episode (0, 1-3, 4+)
- RUB (Resource Utilisation Bands) using the John Hopkins ACG system
- Oncology registration (yes/no?)
- Body Mass Index (BMI) - where available
- Physical activity levels (low (60 minutes/week), moderate (60-149 minutes/week), high (>= 150 minutes/week), no activity, unknown activity levels).
- The following chronic conditions (where more than 20 members included in our survey) were registered for this specific condition:
- Ischemic Heart disease, Hypercholesterolemia, Congestive cardiac failure, Cardiomyopathy, Essential hypertension, Diabetes mellitus, Hypothyroidism, Ulcerative colitis, Human immunodeficiency virus, Systemic lupus erythematosus, Rheumatoid arthritis, Chronic renal failure, Epilepsy, Glaucoma, Depression/Bipolar, Chronic obstructive pulmonary disease, Asthma and Conduction disorder
Which factors increase one's risk of developing long COVID symptoms
Figure 3 represents the output from the multivariate logistic regression analysis for members reporting four or more long COVID-19 symptoms (19% of all respondents). We find that:
- Women are at higher risk: Compared to men, women had a 1.76-fold higher risk of reporting long COVID-19 symptoms
- ICU admission ups risk: Members who were admitted to ICU during their acute COVID-19 infection had a 1.73-fold higher risk of reporting long COVID-19 symptoms, compared to members who did not go to ICU.
- Morbidity ups risk: Complex members i.e., members in a high resource utilisation band (RUB) which refers to a very high morbidity level, had a 2.06-times higher risk of reporting long COVID-19 symptoms compared to RUB 0 i.e., non-users
- Pre-existing conditions up risk: Members with pre-existing chronic conditions were at higher risk of reporting long COVID-19 symptoms, than members without such conditions
- Hospital admission ups risk: Members never admitted to hospital for COVID-19 had a 0.59 times lower risk of reporting long COVID-19 symptoms compared to members that needed to be admitted to hospital
- Vaccination lowers risk: Members that received their second vaccine dose after their initial COVID-19 infection were at 17% lower risk of reporting long COVID-19 symptoms
- Exercise lowers risk: People who had high levels of physical activity before they were diagnosed with Covid-19, exercising for more than 150 minutes a week, were 47 percent less likely to report four or more lingering symptoms after their initial infection. Those who were moderately physically active, and exercised from 60 to 150 minutes a week, were 36 percent less likely to report long Covid-19
These results were statistically significant at the 95% confidence level.
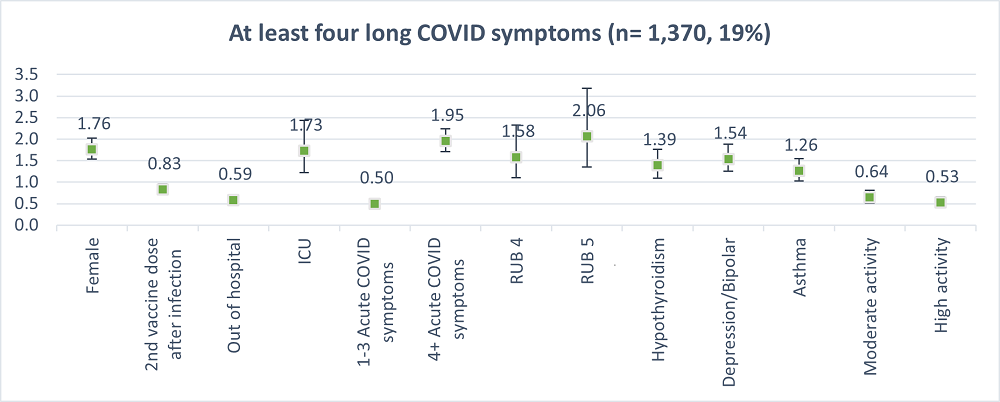
Figure 3: Model outputs for members that reported at least four of symptoms post COVID-19 recovery
We also analysed the most reported long COVID-19 symptoms separately (Figure 4), excluding headaches. Figure 4 shows these results.
In summary, whether we look at individual long COVID symptoms or groups having four or more long COVID symptoms (Figure 3), the risk factors we identified above for developing long COVID recur across each symptom (only with some variation where a chronic condition is involved). This reinforces the consistency of our data on risk factors associated with long COVID symptoms.
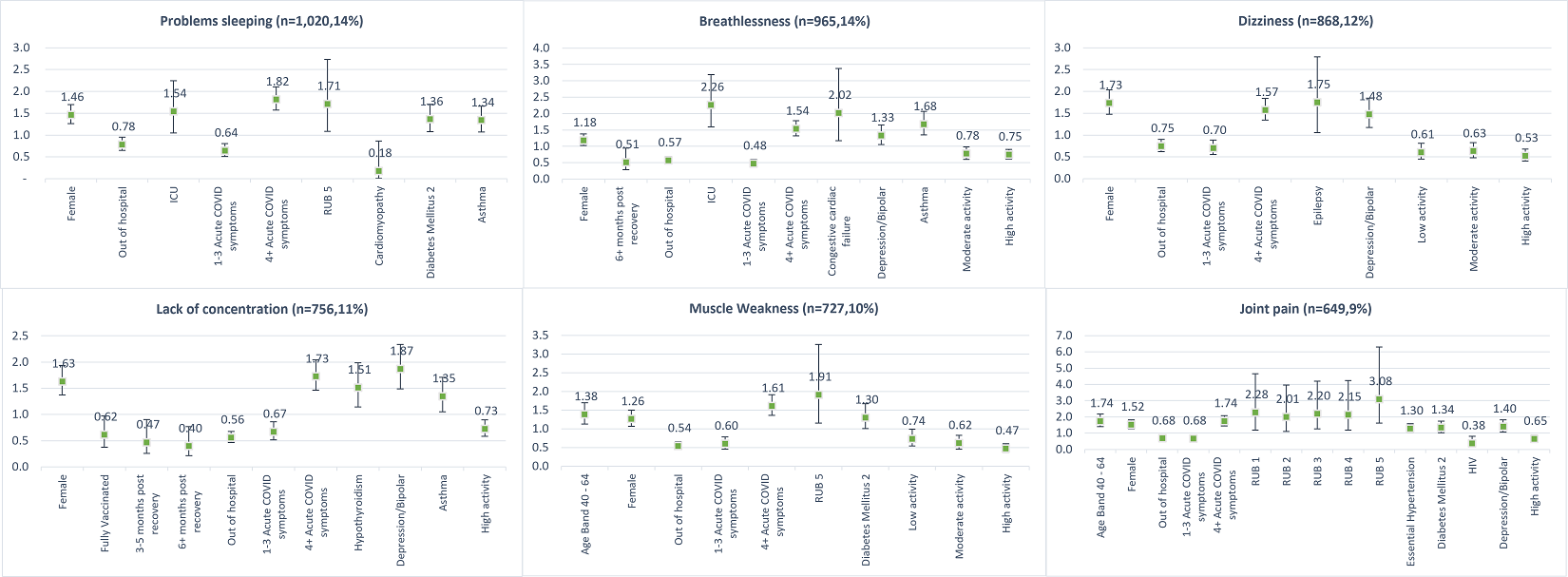
Figure 4: Model outputs for each unique long symptom post COVID-19 recovery
Which factors increases the risk of experiencing a deterioration in ability to perform at least one activity of daily living
Figures 5 and 6 show the outputs of the multivariate logistic regression analysis for members (43% of respondents) reporting a deterioration in at least one activity of daily living.
Figure 5 shows that:
- Women had a 1.88-fold risk of reporting a deterioration in activities of daily living compared to males
- Members who had four or more symptoms during their acute COVID-19 infection had a 1.85 times higher risk of reporting a deterioration in activities of daily living compared to members with no reported symptoms
- Members who didn't need hospitalisation during their acute COVID-19 infection had a 0.47-times lower risk of reporting a deterioration in activities of daily living
- Members admitted to ICU during their acute COVID-19 infection had a 2.64 times higher risk of reporting a deterioration in activities of daily living compared to those with no ICU admission
- Members with pre-existing chronic conditions also having a higher risk for reporting a deterioration in activities of daily living
- COVID-19 vaccination lowers risk: Members who were fully vaccinated prior to their initial COVID-19 infection were at 31% lower risk of reporting deterioration of activities of daily living
- Exercise lowers risk: People who had high levels of physical activity before they were diagnosed with Covid-19, exercising for more than 150 minutes a week, were 28% less likely to report a deterioration in activities of daily living after their initial infection. Those who were moderately physically active, and exercised from 60 to 150 minutes a week, were 20% less likely to report a deterioration
These results were statistically significant at a 95% confidence level.
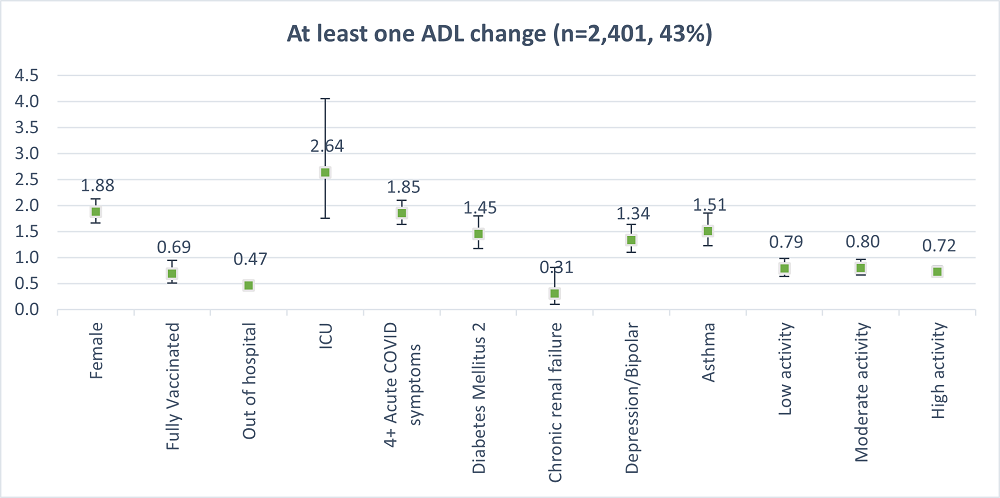
Figure 5: Model outputs for members who reported at least one deterioration in an activity of daily living
Figure 6 shows the results of our analysis of impact on activities of daily living, with the risk factors we identified above as linked to developing long COVID. We see consistency in the risk factors we identified, with some variation only where a chronic condition is involved. In other words, we see strong recurrence in the risk factors we have identified, across impact on activities of daily living.
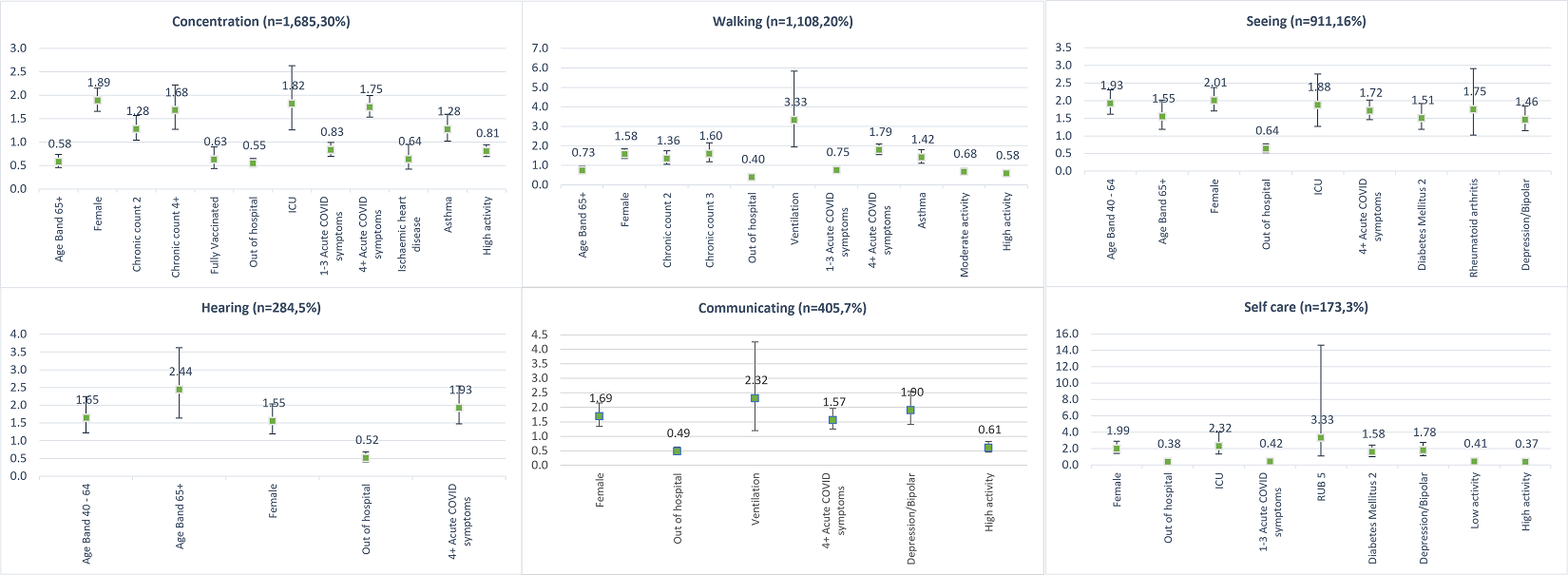
Figure 6: Model outputs for each activity of daily living
In summary
Our analysis adds to the growing body of global research into post COVID conditions.
We see medical scheme members reporting multiple, persistent symptoms after recovering from acute COVID-19 infection.
We found some symptoms reported more often than others. (e.g., headaches). Symptoms were also more likely to occur soon after recovery - within the first two months - rather than further on.
Our modelling shows that being female, having been admitted to ICU during the acute phase of one's COVID-19 infection, and the presence of pre-existing chronic conditions all are associated with increased risk of experiencing post COVID conditions. Nearly 1 in 5 respondents (19%) reported experiencing four or more symptoms for several months following recovery from COVID-19.
We also find that some patients report a reduced ability to perform activities of daily living post COVID-19 infection. Here, our modelling shows that being female, having been admitted to ICU during the acute phase of one's COVID-19 infection, experiencing four or more acute phase symptoms, and the presence of pre-existing chronic conditions all are associated with increased likelihood of experiencing a decline in the ability to perform day-to-day activities.
We will continue to monitor the post-COVID condition landscape and report back on this front again in due course.
Acknowledgements
We wish to acknowledge Dr Geraldine Timothy and Dr Noluthando Nematswerani for their assistance and clinical review of the survey instrument, Brian Klompas for managing the distribution of the survey, and the Business Intelligence and Question Mark teams at Discovery Health. We would like to thank Dr Waasila Jassat - National Health Laboratory Services (NHLS), National Institute for Communicable Diseases (NICD) - and the NICD for the use of their survey instrument and their collaboration.
References
- Mendelson, M., Nel, J., Blumberg, L., Madhi, et al. (2020). Long-COVID: An evolving problem with an extensive impact. South African medical journal, 111(1), 10-12.
- Carfi A, et al. (July 9, 2020) Persistent symptoms in patients after acute COVID-19. JAMA.
- WHO (6 October 2021) - A clinical case definition of post COVID-19 condition
- CDC (May 5, 2022) Long COVID or Post-COVID Conditions
- Mayo Clinic Staff (Oct. 22, 2021) COVID-19 (coronavirus): Long-term effects
- Ganesh R (Jul 16, 2021) Post-COVID Recovery
- Dryden, Murray Thomas Goble and Mudara, Caroline and Vika, Caroline and Blumberg, Lucille and Mayet, Natalie and Cohen, Cheryl and Tempia, Stefano and Parker, Arifa and Nel, Jeremy and Perumal, Rubeshan and Groome, Michelle and Conradie, Francesca and Ndjeka, Norbert and Sigfrid, Louise and Merson, Laura and Jassat, Waasila, Post COVID-19 Condition in South Africa: 3-Month Follow-Up after Hospitalisation with SARS-CoV-2. Available at SSRN: https://ssrn.com/abstract=4007183 or http://dx.doi.org/10.2139/ssrn.4007183
All information shared on this page is based on perspectives gained from analysing data acquired by Discovery Ltd and its various affiliate entities (Discovery). The analysis, which is conducted by Discovery's actuarial and data science team, aims to encourage industry dialogue. Publications containing our analyses are shared for educational and informational purposes only. Each publication reflects only the data available for analysis at the time of publication. It does not, unless otherwise indicated, constitute peer-reviewed, published scientific research, and hence should not be interpreted as such or used as a basis for altering treatment decisions. While every effort has been made to ensure the accuracy of the content conveyed, we cannot be held liable or responsible for any actions or decisions taken based on the information shared in this article.
Interested in knowing more or reporting on these findings?
Please contact us on MEDIA_RELATIONS_TEAM@discovery.co.za to request any updated data available since publication and any further context needed.
Did you find this post useful?
Read our related post on the creation of the Discovery Health COVID-19 Resilience Index. This index predicts an individual's resilience to developing serious COVID-19 illness and is open to the public.

5 min read
New study published in British Journal of Sports Medicine: Exercise protects against serious COVID-19 outcomes
10 February 2022
Authors: Lizelle Steenkamp (Senior Healthcare Statistician at Discovery Health)

11 min read
Discovery Health releases at-scale real-world analysis of Omicron outbreak; including collaboration with the SA Medical Research Council (SAMRC) to analyse vaccine effectiveness
14 December 2021
Discovery Health, South Africa's largest private health insurance administrator, releases at-scale real-world analysis of Omicron outbreak based on 211 000 COVID-19 test results in South Africa, including collaboration with the SA Medical Research Council (SAMRC) to analyse vaccine effectiveness.

11 min read
Pfizer vaccine's real-world effectiveness in protecting against COVID-19 admission and death in the Discovery Health client population
03 November 2021
Authors: Shirley Collie (Chief Healthcare Analytics Actuary, Discovery Health) and Jared Champion (Senior Actuary, Discovery Health)